









SABM
The Benefits of MembershipThe Society for the Advancement of Patient Blood Management (SABM) is an international evidence-based educational resource network of excellence. Our members are comprised of multidisciplinary healthcare professionals who are global leaders in Patient Blood Management. We want to be your partner, your resource, and your mentor. Partner with SABM today and embrace all the resources that SABM has to offer to you and your organization. Join TodayLatest and Greatest
Continue Reading |
 |
 |
|
 |
 |
|
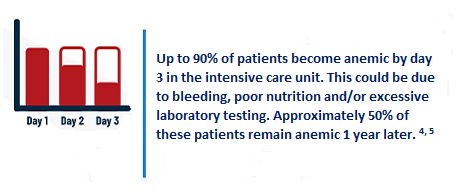
| REFERENCES: 1 Hofmann A et al. Anesth Analg 2022; 135: 511-23. 2 Frank S et al. Anesthesiology 2017; 127: 754-64. 3 Isbisiter JP et al. Anesth Analg 2022; 135: 489-500. 4 Matzek LJ et al. Anesth Analg. 2022;135: 501-10. 5 Warner MA et al. JAMA Netw Open. 2020;3: e2017843. 6 GBD 2021 Anaemia Collaborators. Lancet Haematol. 2023;10: e713-e734. 7 World Health Organization Policy brief 2021. |
ADDITIONAL SOURCES: Anemia Prevention and Management Program Implementation Guide SABM Administrative and Clinical Standards for Patient Blood Management Programs 5th Edition Choosing Wisely® SABM Five Things Physicians and Patients Should Question Warner MA et al. Mayo Clin Proc. 2021;96(12):2980-2990 |

